
Thyroid Hormone and Body Temperature
Why You Should Care About The Relationship Between Thyroid Hormone and Body Temperature

The active thyroid hormone T3 acts on cells - most of which are not in the blood.
T3 is delivered in the blood, as is the precursor T4, which must be converted to T3 to have any effect. Thyroid hormone blood tests can tell us what is in the blood, but nothing more.
The TSH measures a pituitary hormone that increases when the pituitary does not detect adequate levels of thyroid hormones. High TSH is a strong indicator of hypothyroidism, a problem with the gland, but normal TSH is not a good indicator of sufficient T3 activity.
The symptoms of hypothyroidism are largely caused by low T3 activity, though not entirely, as elevated TSH and other factors can cause symptoms and disease. Low T3 activity is the main problem you need to address to resolve hypothyroid symptoms.
The common tests for hypothyroidism cannot assess T3 activity, what’s happening in cells; other diagnostic tools are needed to assess this.
Today, hypothyroidism is assessed by TSH and T4, and, for the most part, treated with T4 (levothyroxine).
This paradigm holds many false assumptions about the diagnosis and treatment of hypothyroidism proper, and also low T3 activity.
Hypothyroidism proper—the failure of the thyroid gland to produce enough thyroid hormones—is only one cause of low T3 activity.
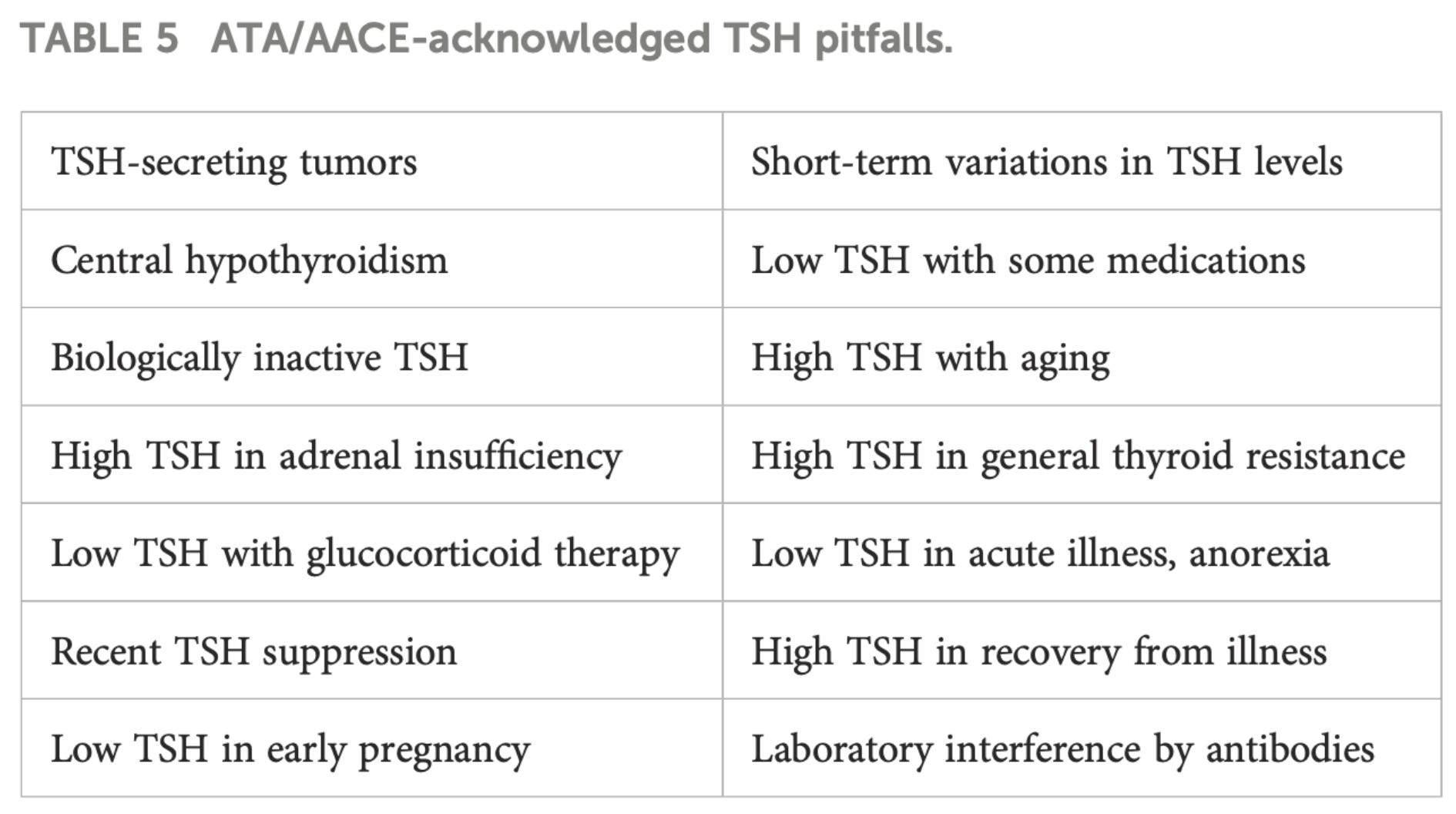
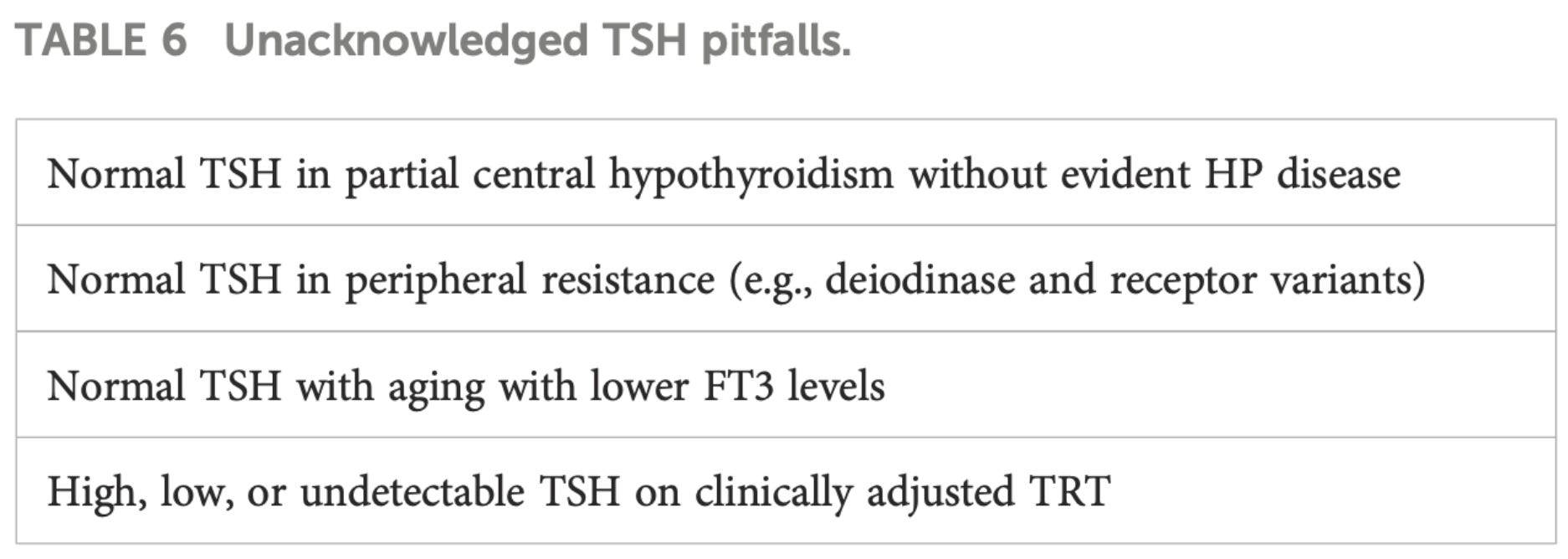
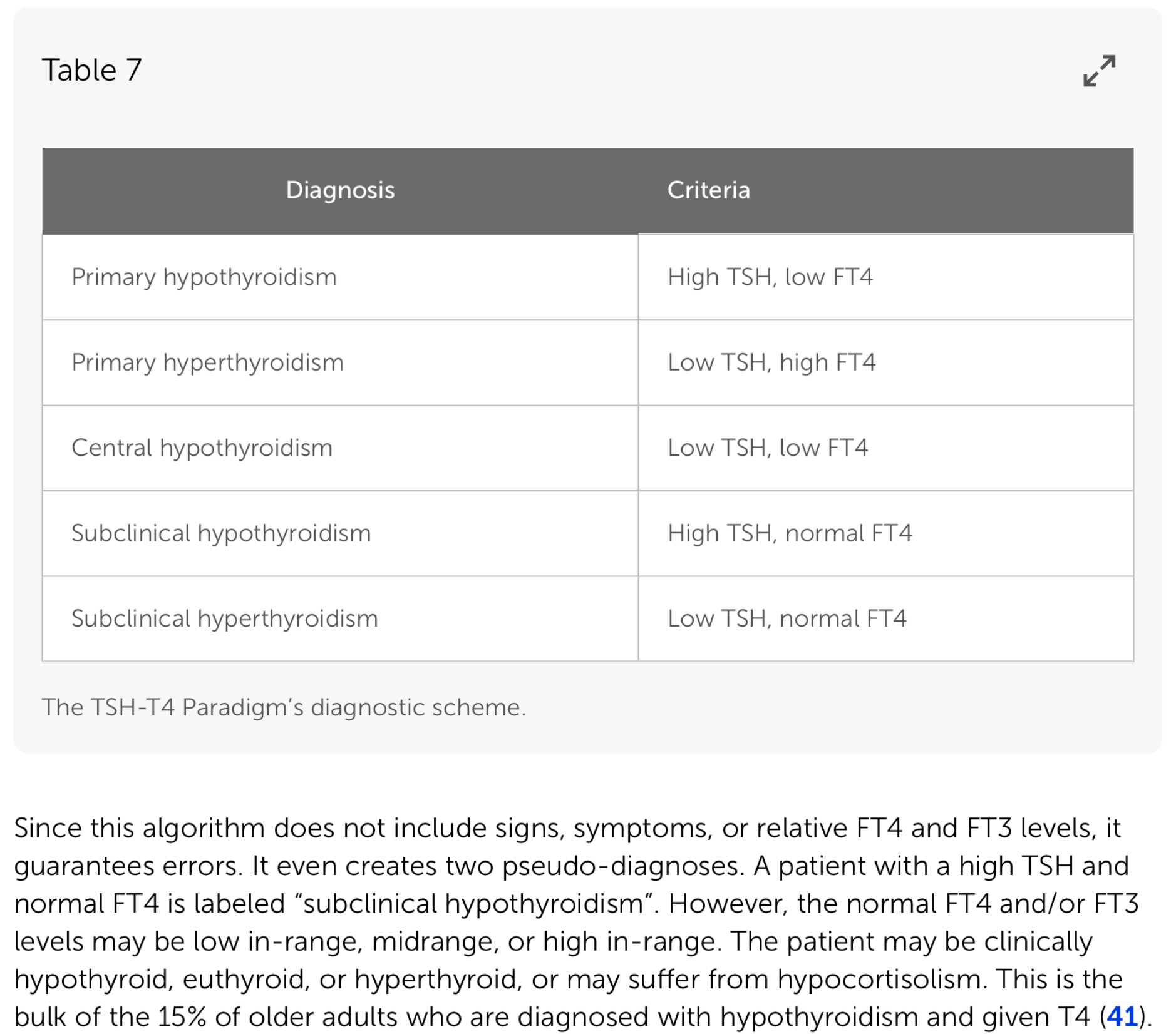
The article Clinical thyroidology: beyond the 1970s’ TSH-T4 Paradigm, outlines many of these false assumptions in detail, revealing why modern diagnostic and treatment protocols leave a lot to be desired. Images below are from that article.
Body temperature is of special interest here because it is a key indicator of T3 activity.
The Basal Metabolic Rate Test
We began to understand hypothyroidism in the latter part of the 19th century, though the disease has been known for thousands of years.
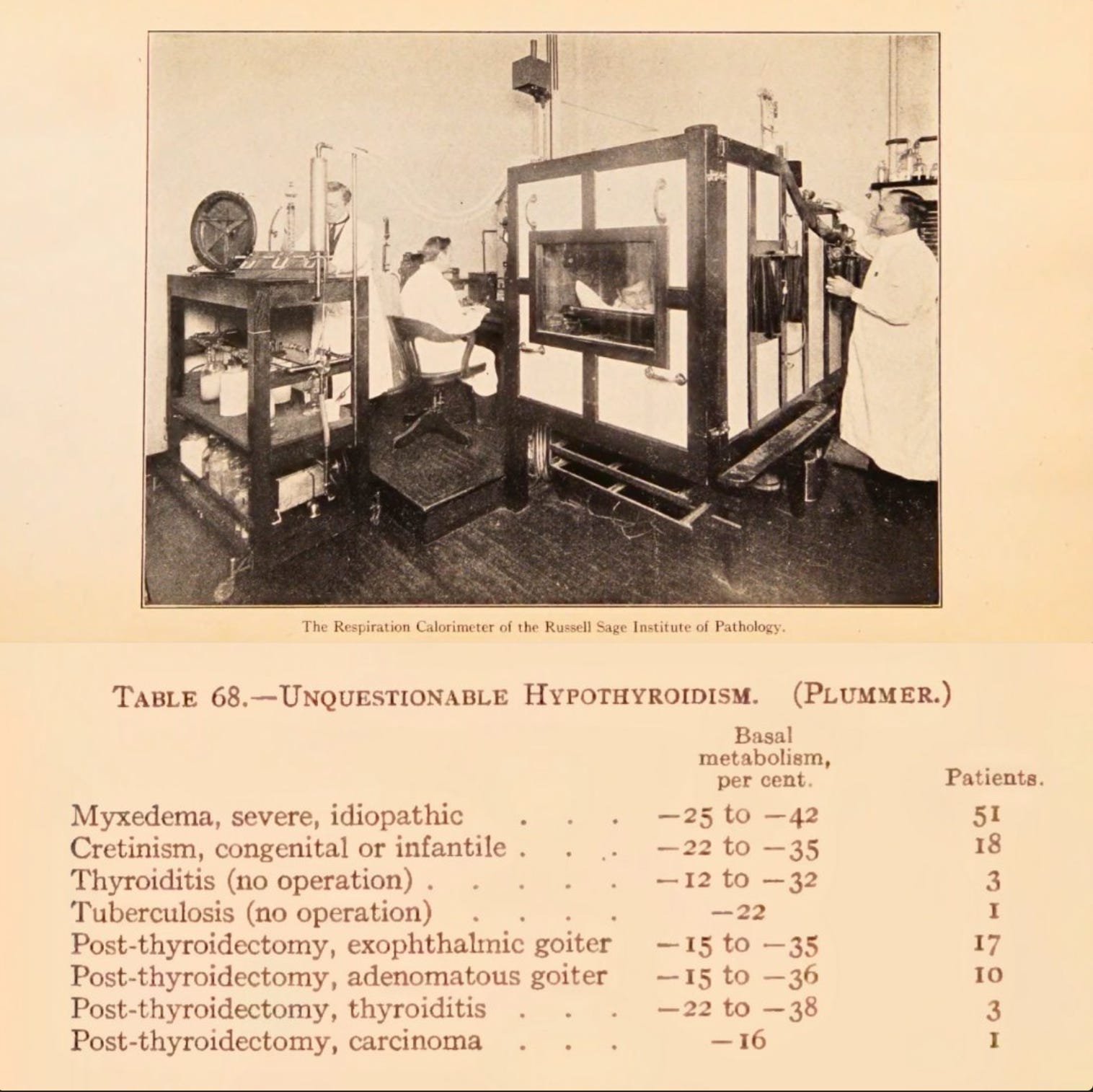
The Basal Metabolic Rate (BMR) test was first used in the 1890s. The BMR test measures changes in oxygen and CO2, which are markers of energy metabolism. It was found that myxedema, the extreme manifestation of hypothyroidism, presented with much lower BMR. No surprise, given the central role of T3 in energy metabolism.
Problems With The BMR Test
The BMR test must be performed at rest; the patient must be calm and undisturbed for it to be fully accurate.
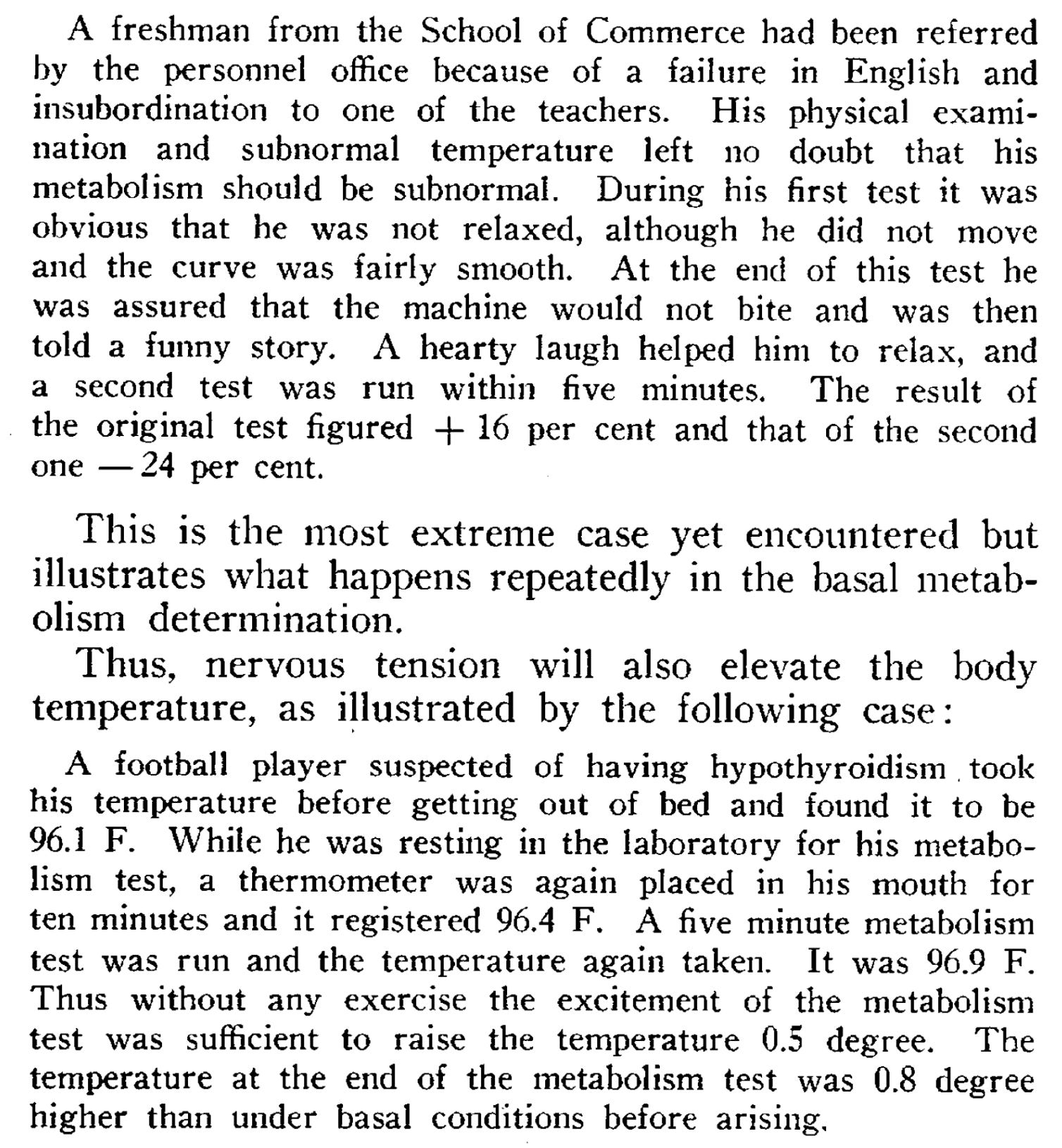
Exercise, digestion, stress, or tension can give a very inaccurate result. It is, then, prone to error, as well as being inconvenient and expensive.
The test caught the attention of Broda Barnes, MD, one of the most influential figures in this field. He found a 40% variance in the test results, depending on whether the subject was relaxed or tense.
Barnes noted some of the BMR’s shortcomings and he was also aware of the influence of thyroid hormone on body temperature regulation. Something well summarized in a recent paper:
“Approximately two thirds of resting metabolic rate is expended in meeting the requirement of the maintenance of a constant body temperature of about 37°C (98.6°F).
In truly sedentary humans where resting metabolic rate is 80% of total energy expenditure, this means that more than 50% of total energy expenditure is dedicated to maintaining this constant core temperature. In normally active humans where the resting metabolic rate accounts for 56% of total energy expenditure, approximately 37% of total energy output is expended in the maintenance of homeothermy.”
“This metabolic energy required for homeothermy is thyroid dependent and apparently generated principally in mitochondria throughout the body of warm-blooded animals.”
[From: Is obesity associated with lower body temperatures? Core temperature: a forgotten variable in energy balance.]
The Response to NDT
Barnes treated hypothyroid patients with NDT, and he began his practice long before the modern blood tests were available.
In a 1942 paper, he reported his observations on individuals treated with NDT, according to symptoms, while undergoing BMR testing or basal temperature testing, a reading of the underarm temperature taken right after waking.
NDT is Natural Desiccated Thyroid USP, often known as Armour. NDT differs significantly from levothyroxine (T4) because it also contains some of the active thyroid hormone T3. A properly dosed regimen of synthetics usually works just as well. T3 is the differentiating factor.
Barnes found that basal temperature was a better predictor of a positive response to NDT in patients with symptoms he believed were caused by hypothyroidism—meaning low thyroid hormone activity—but that were generally not considered symptoms.
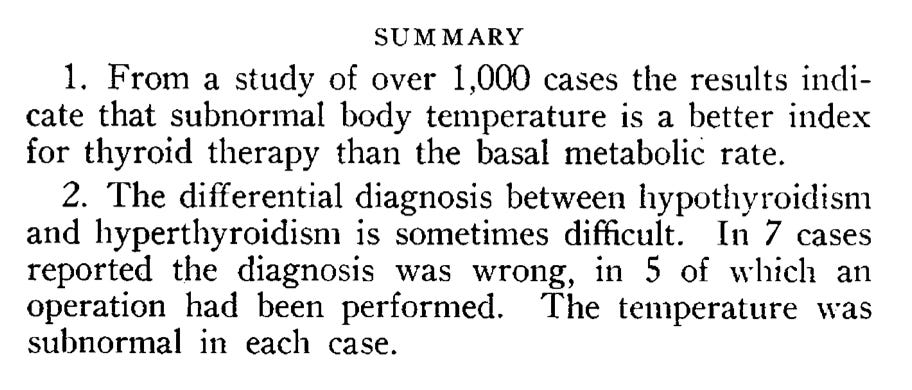
“In August 1942, I could report in The Journal of the American Medical Association on a study with one thousand college students whose basal temperatures were taken and who also received basal metabolism tests. The study indicated that a subnormal body temperature is a better index of hypothyroidism and the need for thyroid treatment than the basal metabolic rate.”
— Broda Barnes
The Basal Temperature Test
Broda Barnes developed the basal temperature test in the 1940s. He used this method very effectively with a large number of patients to assess thyroid hormone status and guide thyroid hormone supplementation with NDT.
The basal temperature differs from an everyday temperature reading in that the entire body must be completely at rest, and the test is done first thing in the morning, in bed, right after waking.
Barnes found that common, low-grade infections, like sinusitis, which can go unnoticed, could artificially raise oral temperature and yield less accurate readings, and so suggested armpit readings.
Temperature varies when measured at different parts of the body; the armpit is about 0.7 °F (0.4 °C) below oral temperature. Temperature also fluctuates over the course of the day, so temperatures at other times and from different places are not equivalent to the basal temperature.
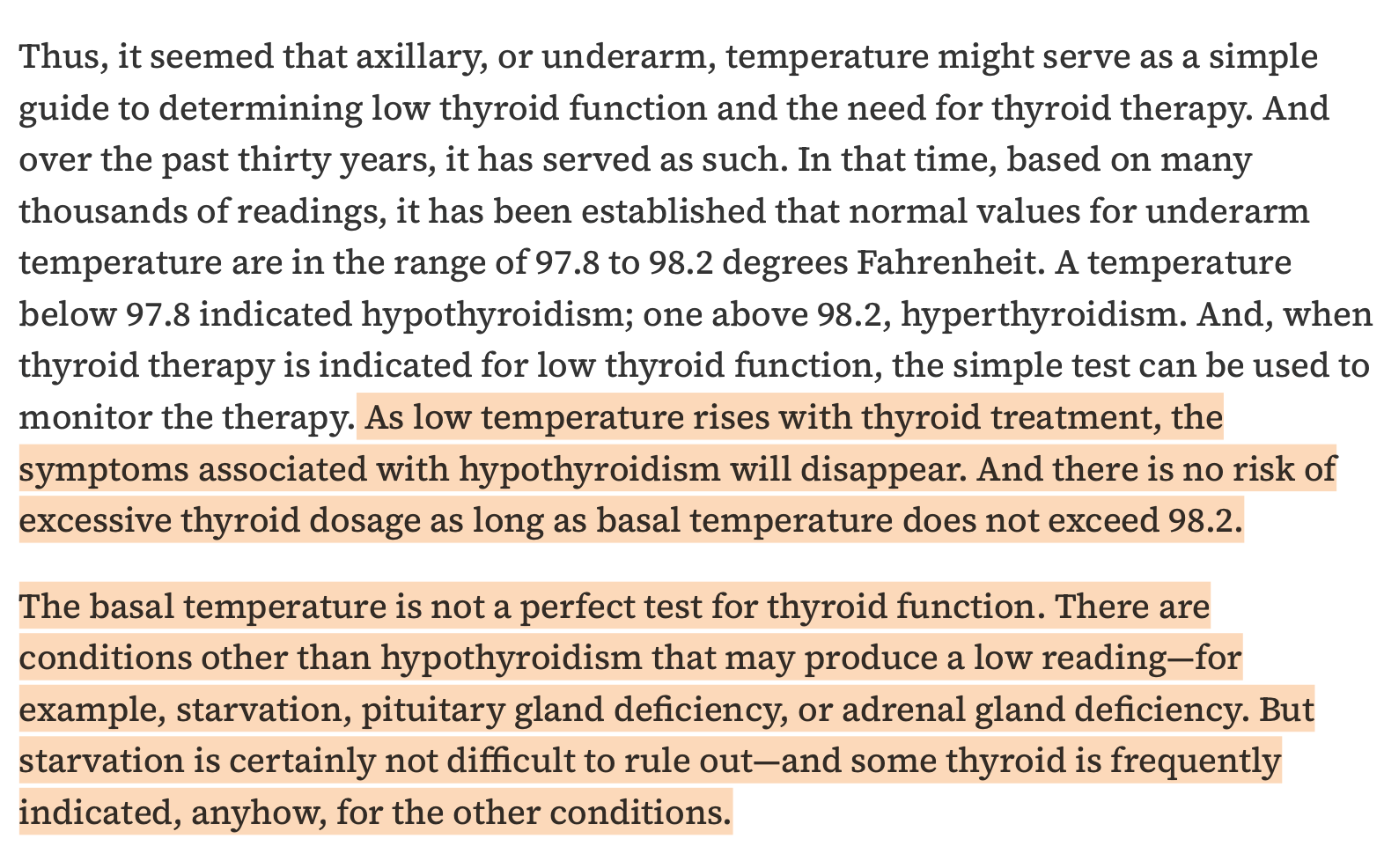
Normal basal temperature is between 97.8 and 98.2 °F (36.5–36.8°C).
This is a little lower than the optimal midday/afternoon temperature.
A basal armpit temperature below 97.8 suggests hypothyroidism (low T3 activity); one above 98.2 can indicate hyperthyroidism.
Hypothyroidism and hyperthyroidism here refer to the under- or overactivity of T3 in cells, not to the output of the thyroid gland or the TSH response.
Barnes had better results correcting the temperature with NDT than those produced by the current method of treating TSH with levothyroxine.
Basal Temperature In Women
Basal temperature varies throughout the menstrual cycle. Women’s temperatures peak just before menstruation and are lowest at ovulation.
So, during menstrual years, basal temperature is best recorded on the second and third days after menstruation begins. Before menarche or after menopause, it can be taken any day.
Birth control pills/HRT override the natural hormonal fluctuations that underlie basal temperature changes. Because every hormonal pill either abolishes the early-follicular temperature trough or replaces it with a uniformly elevated or erratic baseline, Barnes’s basal-temperature test cannot reliably reflect thyroid hormone status in pill users.
The Effects of Stress on Body Temperature
Ray Peat, Ph.D., was strongly influenced by Barnes’ work on hypothyroidism and added to it by noting the effect of stress on body temperature.
Peat’s definition of stress includes, but is not limited to, psychological stress, and is rooted in the physiological changes induced by various environmental factors, as evidenced by alterations in cortisol, adrenaline, nitric oxide, serotonin, and free fatty acids. Stress in this context encompasses more than just feeling stressed.
Peat’s definition of stress and the intricacies thereof are not the topic here, but suffice to say that factors unrelated to thyroid hormone activity that Barnes did not fully explain also alter basal temperature.
If someone has clear hypothyroid symptoms, but the basal temperature reading does not concur, Peat suggested looking at the temperature response to food, as food lowers stress, and this could indicate that stress was keeping the temperature up.
“In a normal person, both temperature and pulse rate rise after breakfast, but in very hypothyroid people either, or both, might fall.”
— Ray Peat.
Electric blankets, hot and humid weather, infection, and uncoupling agents are some other things that change the context, as do diets where the serum T3 drops, but temperature may be maintained by vasoconstriction or adrenergic thermogenesis—heat produced when adrenaline/noradrenaline activate adrenergic receptors, increasing fuel breakdown and uncoupled mitochondrial respiration to generate heat.
Testing Equipment
Barnes used mercury thermometers that are difficult to get these days. Easily accessible, reasonably priced digital thermometers are unreliable, in my experience, meaning they can give VERY different readings when tested at the same time. The most accurate, affordable solution is a modern, liquid thermometer. The Geratherm Classic is my recommendation, but there are other similar options out there. Look for calibrated Galinstan.
How To Test
For basal readings, keep the thermometer beside the bed. You should reach for it immediately upon waking at your normal time. Place the thermometer deep into the armpit and keep it there for 5 minutes. Then take the reading.
Initially, you should run tests on both armpits. There may be a significant but consistent difference between them. Go with the higher one.
Readings below 97.8 °F (36.5 °C) indicate low thyroid hormone activity.
Over 98.2 °F (36.8 °C) suggests thyroid hormone activity is too high.
The peak temperature should be higher, reaching 98.6°F (37.0°C) sometime in the afternoon.
Remember, though these readings tell us a lot and may be more useful than blood tests for assessing thyroid hormone activity, they are also affected by other factors, so the context must always be taken into account.
For Barnes and Peat, the conclusive test was the symptomatic response to NDT or T3.
Thanks for reading and sharing. If you needto know more about hypothyroidism and low T3 activity then check out my Hypothyroid Masterclass Course where I have a series of videos, all immediately available on demand, covering every aspect of these topics. Link is HERE!
Sources and recommended reading:
Broda Barnes: Hypothyroidism: The Unsuspected Illness
Is obesity associated with lower body temperatures? Core temperature: a forgotten variable in energy balance.
Clinical thyroidology: beyond the 1970s’ TSH-T4 Paradigm
Broda Barnes: BASAL TEMPERATURE VERSUS BASAL METABOLISM
BASAL METABOLISM IN HEALTH AND DISEASE - EUGENE F. DU BOIS, M.D