
Thyroid Hormone and Depression
Depression is a state of low brain energy that can be caused by low thyroid hormone.

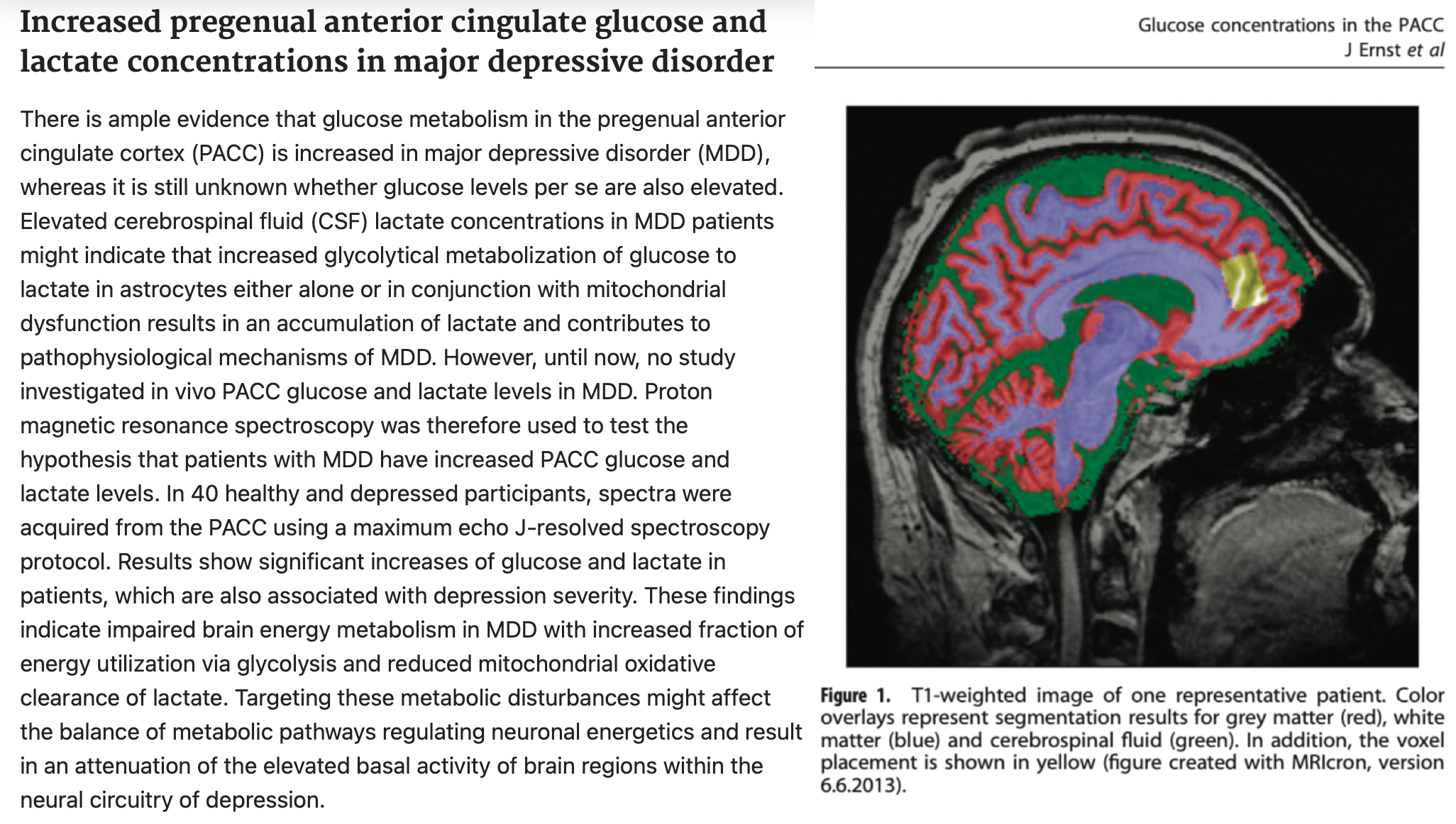
Glucose oxidation is reduced in brain regions associated with depression¹.
This means less efficient use of the brain’s primary fuel, as well as lower CO2, and increased lactate. Lithium, when effective, lowers lactate in these regions in bipolar depression².
—
If you need more help understanding hypothyroidism and low T3 activity then check out my hypothyroid masteclass video series and group here: 📌 skool.com/thyroid 📌
—
Thyroid hormone T3 is needed for optimal glucose oxidation, and low brain metabolism is found in hypothyroidism.
Overall and regional glucose oxidation is reduced in hypothyroidism³.
“Brain hypometabolism is commonly observed in thyroid disorders. Clinical data suggest that there is a significant and global decrease in brain glucose metabolism in severe hypothyroidism of short duration, and that both neural activity and regional glucose metabolism are reduced in the brains of mild-moderate hypothyroid patients (specifically, in hippocampus, bilateral amygdala, anterior, left subgenual, and right posterior cingulate cortex) and restored to control levels following thyroid hormone replacement therapy (Constant et al. 2001; Bauer et al. 2009)... in recent studies it was observed that there are decreases in direct measures of cerebral glucose metabolism, such as the ratio of phosphocreatine to inorganic phosophate, in hypothyroid brains, suggesting that a direct effect of thyroid hormones on brain glucose utilization cannot be ruled out and that changes in vascular resistance may be secondary to decreased cerebral metabolism.”
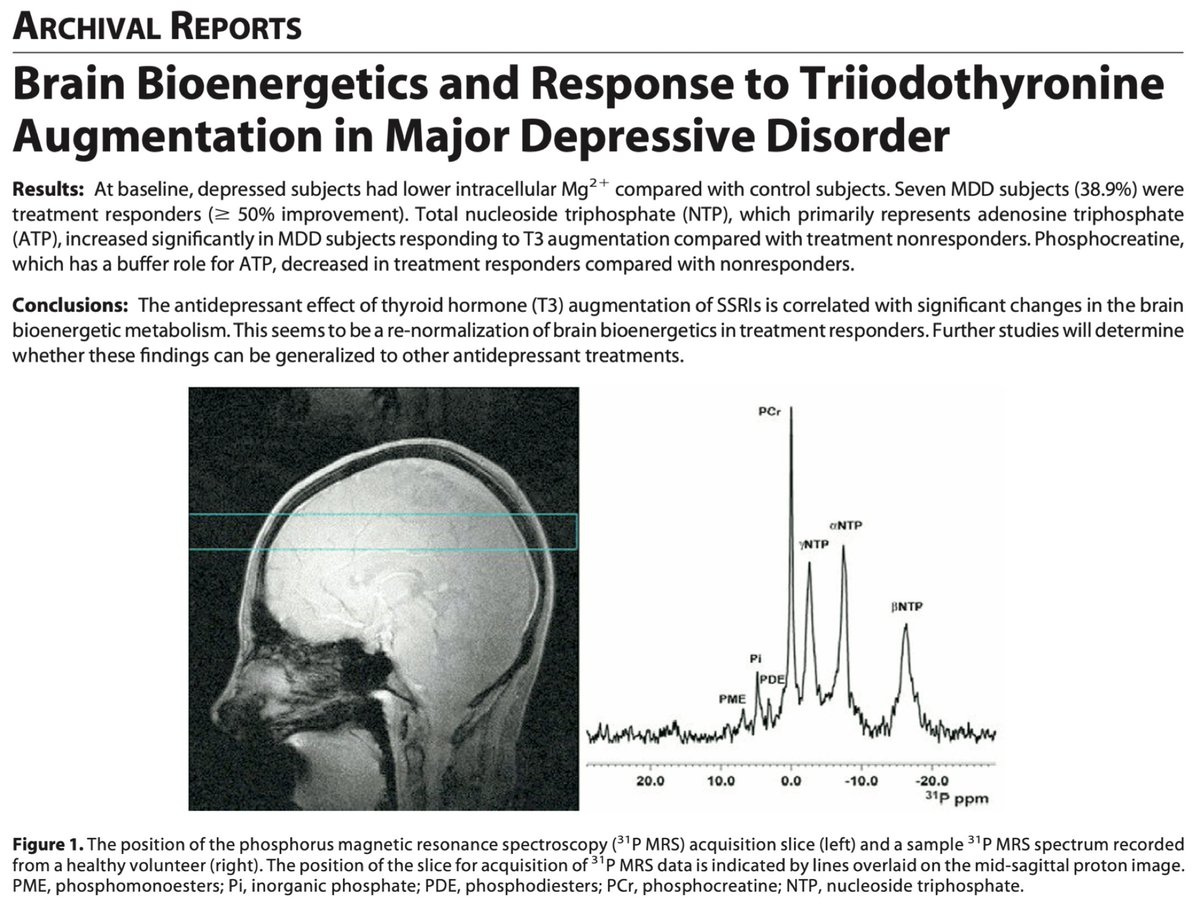
Thyroid hormone T3 supplementation has antidepressant effects which track with improvements in brain energy, according to research in people with “antidepressant resistant” depression⁴.
“The antidepressant effect of thyroid hormone (T3) augmentation of SSRIs is correlated with significant changes in the brain bioenergetic metabolism. This seems to be a re-normalization of brain bioenergetics in treatment responders.”
Depression was long known to be a common symptom of hypothyroidism, though this is often overlooked now due to serotonin and psychological theories, and misunderstandings regarding the accuracy of modern thyroid blood tests⁵.
“Depression has been the major affective illness described in hypothyroid patients. It has long been recognized that there is a strong relationship between thyroid disorders, particularly hypothyroidism, and disturbance in mood.”
Blood tests don’t accurately reflect what’s happening in tissues and organs, especially the brain.
“The active thyroid hormone in the brain is T3. The relative hypothyroidism localized to the brain may be secondary to inhibited activity of the D2 enzyme, which is responsible for the conversion of T3 to T4.”
“Psychiatric presentations (of hypothyroidism) include cognitive dysfunction, affective disorders, and psychosis. The realization that hypothyroidism might be the potential etiology of an assortment of symptoms is critical in the identification and treatment of the hypothyroid patient. Once hypothyroidism is identified, symptoms usually respond to appropriate thyroid hormone supplementation.”
[Hypothyroidism Presenting as Psychosis: Myxedema Madness Revisited]
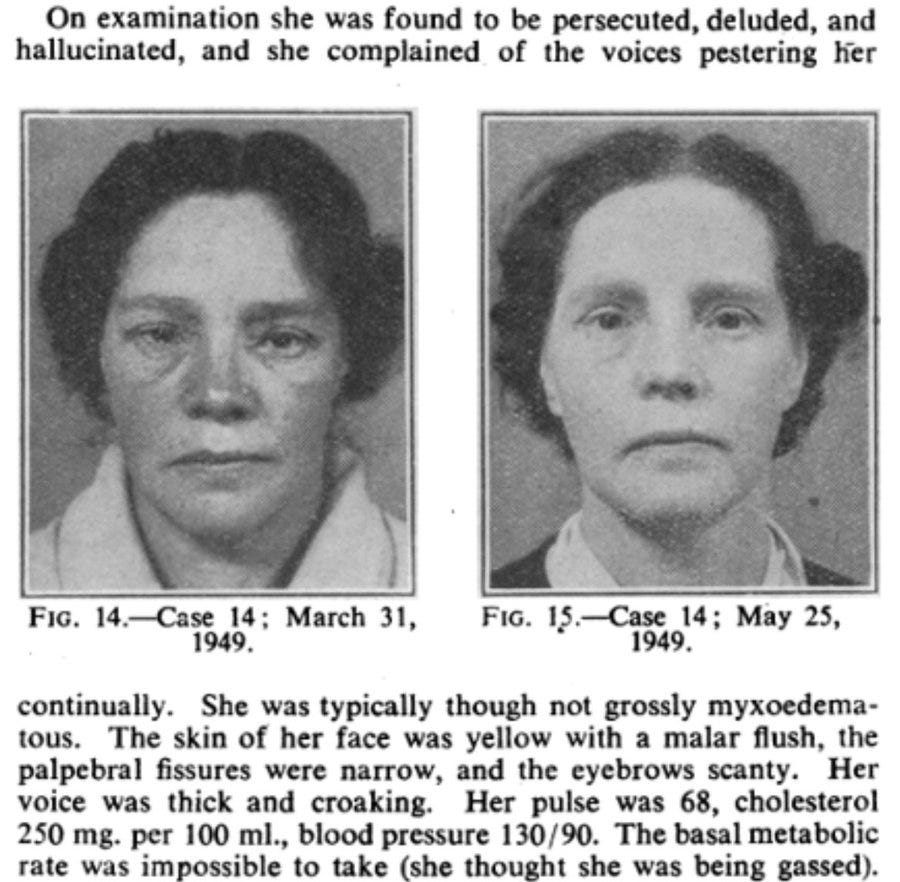
“On examination she was found to be persecuted, deluded, and hallucinated, and she complained of the voices pestering her continually. She was typically though not grossly myxoedematous. The skin of her face was yellow with a malar flush, the palpebral fissures were narrow, and the eyebrows scanty. Her voice was thick and croaking. Her pulse was 68, cholesterol 250 mg. per 100 ml., blood pressure 130/90. The basal metabolic rate was impossible to take (she thought she was being gassed). Progress.—She was started on thyroid, ‡ gr. thrice daily, increased five days later to 1 gr. thrice daily. Within a fortnight there was an obvious facial change and she began to have insight into her hallucinations-admitting they were not real voices though she still heard them. After three weeks the cholesterol had come down from 250 to 120 mg., the hallucinations had stopped, and she said, “I feel different, I see things different, and my husband says I look younger. I talk different; I’ve lost that deep tone and seem to speak lighter.” She was discharged a month after admission and continues to attend as an out-patient in normal physical and mental health. Soon after discharge, when she went to her grocer he said to her : “Are you a relation of the Mrs --- who used to come in here and went to hospital? “ He had completely failed to recognize her.”
Testing for thyroid issues usually focuses on TSH and T4. T4, also called levothyroxine or Synthroid, is the precursor to the active thyroid hormone T3.
T4 must be converted to T3 to have any beneficial effect, and many people have suboptimal conversion.
But many people with depression have suboptimal T3 in the blood, and low T3 is even more likely as depression worsens.
TSH can increase as thyroid hormone (T3) supply to tissues and organs fails, and this is usually ignored if the T4 is within the normal range. The reasoning is that the thyroid is still producing enough T4 to keep things in the normal range, and the incorrect assumption is that this leads to an adequate thyroid hormone T3 supply.
“We found a decrease in T3 and an increase in TSH levels amongst mild, moderate and severe grade of depression patients.”
“Evaluation of thyroid status prior to antidepressant therapy is suggested.”
“This suggests subclinical hypothyroidism in most patients which could lead to non-responsiveness to the conventional antidepressant therapy.”⁶
The most common test for thyroid issues is TSH. TSH is a pituitary hormone that responds to thyroid hormone levels in the blood, among other things. It is heavily influenced by stress and diet, independent of thyroid hormone T3 status.
People taking T4 are more likely to be depressed if their TSH is in the upper part of the ✧normal✧ range.
T4 (levothyroxine/Synthroid) is the most common thyroid hormone medication. It’s not a great way to optimise thyroid hormone T3, and the normal TSH range doesn’t help assess thyroid hormone status.
“Considering that hypothyroidism and depression share some clinical features, some researchers use the “brain hypothyroidism” hypothesis to explain the pathogenesis of depression.”
The upper cutoff for TSH is usually around 4.5. In other words, many people will be told that they don’t have a thyroid issue unless it is over 4.5. But people on T4 with TSH above 2.5 are more likely to be depressed.
“The present study identify a TSH value of 2.5 mU/L as the optimal cut-off point to predict depression symptoms in hypothyroid patients treated with T4.” ⁷
In “treatment resistant” depression - where two or more antidepressant drugs fail - thyroid hormone T3 can be effective - even in people with normal thyroid blood tests.
“Up to 100 million individuals globally might have treatment resistant depression (TRD) according to epidemiologic studies.”
“A 48-year-old white perimenopausal woman with obesity (body mass index: 34 kg/m2) and hypertension presented to the outpatient psychiatric clinic seeking treatment for chronic clinical TRD. She had been in several failed medication trials over the last 2 years, including SSRIs, serotonin-norepinephrine reuptake inhibitors, bupropion, lithium, olanzapine, aripiprazole, and Adderall. She was currently on daily bupropion XL 450 mg, fluoxetine 40 mg, and aripiprazole 15 mg for over a year, but still reported low mood with mild reactivity and lack of motivation, high appetite, hypersomnia, and lack of concentration.
All laboratory values were within normal range, including thyroid function test.
The patient was given a trial of a small dose of T3 liothyronine 10 µg, and after 2 weeks, the dose was increased to 25 µg/d. Within 4 weeks, the patient reported a significant change in her mood, motivation, energy, concentration, and cognitive function with no side effects (PHQ-9 score <7). Thyroid function tests, including T3, T4, rT3, and TSH, followed up after a 1-month and 6-month period, were all within normal range, and no physical or mental adverse effects were reported after 6 months of T3 treatment.”⁸
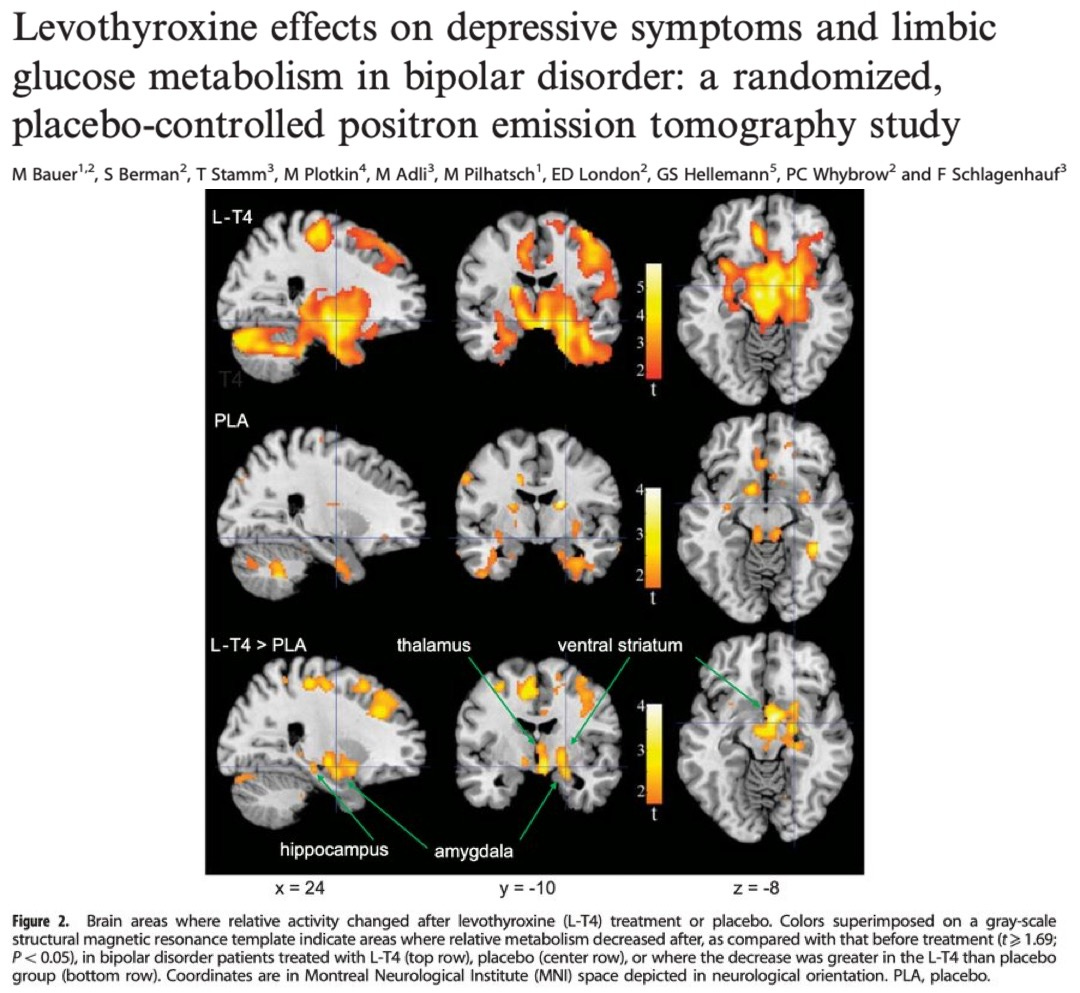
High doses of T4 have been used in bipolar depression. T4-only is not the best way to optimize thyroid hormone T3 due to conversion issues, but it shows that even levothyroxine can improve outcomes in people with severe thyroid hormone metabolism issues.
“Administration of supraphysiologic thyroid hormone improves depressive symptoms in patients with bipolar disorder by modulating function in components of the anterior limbic network.”⁹
Papers are reporting no effect from thyroid hormone in depression, some of them even use the thyroid hormone T3.
These studies give every patient the same dose, or dose to TSH - they can’t be used to conclude anything because they are not properly assessing or treating the suboptimal T3.
This is analogous to giving a group of type 1 diabetics the same dose of insulin, or an insulin precursor that they may or may not be able to convert to insulin, and using the results to make conclusions about the efficacy of insulin in T1D.
A report using a more rational approach, dosing combination T3 and T4 to achieve free T3 in the upper 20% of the normal range while keeping the TT3/RT3 at 10:1 or better, reported an average improvement of 46% in depression.
TT3 is the total T3 in the blood. RT3 is an inactive metabolite of T4. A lower ratio TT3/RT3 indicates poorer conversion and suboptimal treatment.
“R.C. is a 47 year-old male, total thyroidectomy (papillary carcinoma), post RAI and on levothyroxine 150mcg/d. He presented with perennial allergies, recurrent sinusitis and bronchitis in spite of repeated antibiotics and steroids both IM and PO. He had many primary doctor visits and was frequently out of work. He was also excessively tired and depressed and on klonopin. I initially treated him with azelastine spray and ordered my thyroid profile: FT3 - 3.3 , TT3/RT3 - 3.7. I Optimized his metabolism on levothyroxine 75mcg plus liothyronine 12.5mcg am/10mcg pm. His thyroid profile on this dosage: FT3 - 4.1, TT3/RT3 - 10.4, TSH - 0.053 (continued suppression needed to repress any papillary thyroid cancer remnants).
He no longer gets sick and is back to work. His excessive tiredness is 100% gone. His depression is 100% gone. He is no longer on klonopin.”¹⁰
Even without patient-tailored dosing, adding some thyroid hormone T3 can improve depression and other cognitive symptoms.
“Among 17 scores on tests of cognitive performance and assessments of mood, 6 were better or closer to normal after treatment with T4 plus T3 (compared to T4 only). Similarly, among 15 visual-analogue scales used to indicate mood and physical status, the results for 10 were significantly better after treatment with T4 plus T3.
In patients with hypothyroidism, partial substitution of T3 for T4 may improve mood and neuropsychological function; this finding suggests a specific effect of the T3 normally secreted by the thyroid gland.”¹¹
To summarize, low thyroid hormone (T3) activity is implicated in depression. T3 is needed for optimal glucose oxidation, which is impaired in depression. Basic TSH/T4 testing and treatment are insufficient, inadequate, and inappropriate for assessing thyroid hormone T3 status. T3 status is what determines hypothyroid symptoms, including depression. Patient-tailored approaches using T3, reverse T3, symptoms, response to thyroid hormones, and basal temperature are often more useful at assessing thyroid hormone metabolism.
Notes:
This does not mean that hypothyroidism or low T3 activity is the only cause of depression, but it certainly is a common, overlooked, and undertreated factor.
Thyroid hormones are powerful substances that should not be taken carelessly, especially T3, which is a fast-acting metabolic stimulant. Inappropriate T4 dosing can suppress thyroid function and worsen symptoms by lowering T3.
—
Thanks for reading, if you need more help understanding hypothyroidism and low T3 activity then check out my hypothyroid masteclass video series and group here: 📌 skool.com/thyroid 📌
—
Sources
¹ Increased pregenual anterior cingulate glucose and lactate concentrations in major depressive disorder
² Increased Brain Lactate During Depressive Episodes and Reversal Effects by Lithium Monotherapy in Drug-Naive Bipolar Disorder: A 3-T 1H-MRS Study
³ Thyroid hormone’s role in regulating brain glucose metabolism and potentially modulating hippocampal cognitive processes
⁴ Brain bioenergetics and response to triiodothyronine augmentation in major depressive disorder
⁵ Hypothyroidism Presenting as Psychosis: Myxedema Madness Revisited
⁶ A STUDY OF THYROID HORMONES (T3, T4 & TSH) IN PATIENTS OF DEPRESSION
⁷ TSH cut off point based on depression in hypothyroid patients
⁸ Triiodothyronine Augmentation for Treatment-Resistant Depression
⁹ Levothyroxine effects on depressive symptoms and limbic glucose metabolism in bipolar disorder: a randomized, placebo-controlled positron emission tomography study
¹⁰ The definition of Optimal Metabolism and its association with large reductions in chronic diseases
¹¹ Effects of thyroxine as compared with thyroxine plus triiodothyronine in patients with hypothyroidism
See ‘Clinical thyroidology: beyond the 1970s’ TSH-T4 Paradigm’ for a good breakdown of the problems with current testing and treatment methodology
Great stuff! Thank you for sharing!
AMEN & HALLELUJAH! I see clients *constantly* with "normal" TSH and sometimes even normal free T3, but the T3 is near the bottom of the range, and ... yep: they can't lose weight, they have low mood, fatigue, etc. I just wish more clinicians were willing to prescribe T3 and treat based on *symptoms* rather than solely the TSH or even the T3 level. I stress this to clients all the time: "Normal does not mean *optimal.*" Unfortunately, as a nutritionist and not a medical professional, I can't prescribe anything, but so many docs are just absolutely in the dark ages when it comes to this. And so many millions suffer because of it. I'm looking to put together a directory of practitioners who prescribe T3 (or even NDT) and really understand the nuances of all this. I need trusted professionals to refer clients to -- and they are hard to come by! Some doctors would be happy to put statins in the water supply, but you practically have to murder someone to get your hands on some T3. It's unconscionable.